

Marcus has been COO of a regional orthopedic group for eleven years. He approved the telehealth platform in 2021. He sat through the implementation kickoff. He watched the utilization numbers climb. And on a Monday morning in March, he is standing at the nurses station listening to four phones ring at once, wondering why nothing actually changed.
Most telehealth investments improved visits, but left patient access broken.
The video visits are happening. The schedule looks fuller than it did two years ago. And somehow his staff is just as stretched, his patients are just as frustrated at the front end, and the calls that should have been handled automatically are still landing on the same two people who have been handling them since 2018.
Marcus does not have a telehealth problem. He has an incomplete telehealth operation. And he is far from alone.
Most practices implemented telehealth by building one part of it and left nine parts untouched. The video visit platform went live. The scheduling tool stayed the same. Triage still ran through whoever answered the phone. Intake forms were still faxed. Refill requests still piled up in a shared inbox. None of it talked to each other, because none of it was ever designed to.
That is not a technology failure. It is a design failure. Telehealth was never built as one coordinated system for most practices. It was built in pieces, each solving a different problem, never quite talking to each other. And somewhere in the middle of all that, a video visit happens. That is not a telehealth operation. That is a video visit with a scheduling problem attached to it.
There is a platform built to unify all ten services a complete telehealth operation requires, connecting every patient interaction from first contact through completed care. That coordination is exactly what practices like EmergeOrtho used to turn a fragmented access operation into measurable ROI: Read about how EmergeOrtho fixed gaps and improved patient access LINK →
Across 15 million patient interactions, that platform delivers a 95–99% completion rate across every channel. That is not a pilot result. It is the operational standard a complete telehealth operation reaches.
What Telehealth Actually Is
Most people define “telehealth” as a video visit with a provider. That is telemedicine: a provider consultation over a real-time video channel. Telemedicine is one part of telehealth, and typically not the highest-volume part.
“Any use of electronic information and telecommunications technologies to support and promote long-distance clinical health care, patient and professional health-related education, and public health and health administration.” — Health Resources and Services Administration (HRSA)
That definition is broader than most practices run with. Every patient interaction that does not require a physical exam is, by that standard, a telehealth interaction. Scheduling a follow-up. Triaging a symptom call. Authorizing a refill. Sending intake paperwork. Coordinating a specialist referral. All of it.
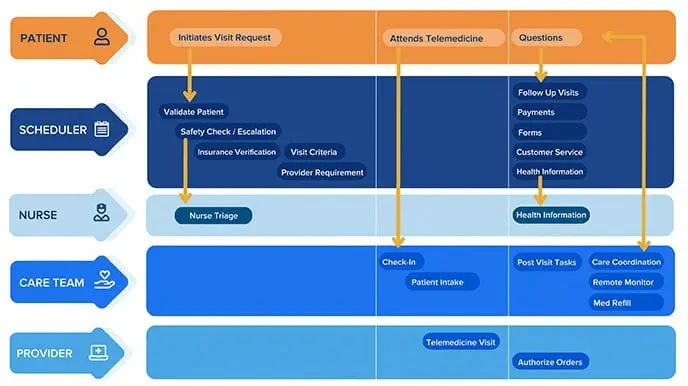
A complete telehealth operation covers ten services. Marcus’s group had three running well. The other seven were either manual, inconsistent, or missing entirely. That is not unusual. That is the norm.
If even a few of these are incomplete, your patient experience breaks, no matter how good your providers are.
- Scheduling visits to completion
- Nurse triage and clinical health guidance
- Telemedicine provider visits
- Medication refill management
- Patient intake and registration
- Care coordination across departments
- Capacity optimization and fill management
- Payment estimates and processing
- Remote patient monitoring
- Demand management and patient engagement
What follows is a walkthrough of all ten, what each one does for your operation, and what it costs you when it is incomplete.
The Access Standard Has Shifted
Before diving into the ten services, it is worth understanding why completing all of them matters now more than it did five years ago.
Patients today choose providers based on how easy it is to access care, not on clinical reputation alone. A 2025 report from the American Medical Association found that 71.4% of physicians were using telehealth weekly by 2024, up from 25.1% in 2018. The infrastructure is there. What patients now expect is that using it feels effortless.
Amazon One Medical now offers on-demand virtual visits for 30-plus common conditions starting at $29, accessible through the same app patients use for groceries and package tracking. In January 2026, Amazon launched a health AI assistant for One Medical members that routes patients directly to providers inside the app. These are not innovations in clinical care. They are innovations in access. And they have raised the bar for what patients expect from every healthcare interaction, including yours.
Walmart raised that bar further when it launched Better Care Services in January 2026, a digital platform connecting its customers to a curated network of third-party providers for urgent care and behavioral health, alongside prescription services through its pharmacy network. This is not Walmart experimenting with healthcare. It is Walmart deploying its logistics infrastructure and customer base to make healthcare access as frictionless as same-day delivery. Patients who book a virtual urgent care visit through Walmart and receive their prescription the same afternoon are going to notice when your operation requires more steps and more friction to accomplish the same outcome.
The risk is not just competition. It is comparison. Patients who have experienced frictionless access elsewhere will notice when your operation requires more effort than it should. Completing all ten services is how you meet patients at the standard they now carry with them.
Marcus noticed this in his own data before he could name it. New patient conversion was softer than it should have been, and follow-through on first-contact scheduling was inconsistent. Patients were reaching out, not completing, and not coming back to try again.
See where your telehealth operation stands today. Most practices are running four or five of the ten telehealth services well. The Keona Patient Service Maturity Assessment identifies exactly where your gaps are and what closing them is worth.
Assess Your Telehealth Maturity Stage
What Patients and Providers Gain When All Ten Services Work
A complete telehealth operation does not just solve an operational problem. It changes the experience on both sides of every patient encounter.
For your patients, a complete operation means choice: the channel they prefer, the time that works for their schedule, and the care team they trust. It means faster access without the transportation barrier that research published in the American Journal of Public Health found disproportionately affects Hispanic patients, Medicaid recipients, and those below the poverty threshold. It means a visit that does not consume the 121 minutes the American Journal of Managed Care documented as the average in-person care day. And it means better outcomes: patients who can access care easily are more likely to complete follow-ups, adhere to treatment plans, and stay engaged between visits.
For your providers and practice, a complete operation means revenue that does not fall off the schedule when a patient cancels or a slot goes unfilled. It means schedule flexibility and care delivery that continues when staff are short or conditions are disruptive. It means departments that share information rather than work around each other. It means a practice that adapts to whatever the competitive landscape requires rather than one that is locked into the model that worked five years ago.
These are not abstractions. They are the outcomes that follow when the ten services are connected rather than fragmented.
Service 1: Scheduling: Your Patients Schedule Themselves. Your Staff Handles What Actually Needs Them.
Scheduling is the entry point for every patient relationship, and it is where most telehealth operations lose more ground than they realize. A patient who cannot schedule easily does not call back. They find somewhere else to go for care.
Your scheduling operation should complete appointments 24 hours a day, across every channel your patients use to reach you. That means automated rules that know which provider, which appointment type, and which slot is correct for each patient request, without a staff member manually making that determination on every call.
When Marcus pulled his data, his two front-desk staff were spending an average of 22 minutes per new patient getting through scheduling, intake, and insurance verification. Manually. On the phone. For every patient. The telehealth platform had not touched any of that.
Your schedule fills accurately without manual oversight. For patients who call, your phone AI handles the inbound request and routes it to the right appointment type without staff intervention. For patients who prefer to schedule on their own time, your web and self-service tools complete the same workflow online or through your patient portal. Your waitlist converts cancellations back to completed visits before your staff sees them, and your patients book on their timeline, not yours.
Transportation is a documented barrier to scheduling completion. A 2020 study in the American Journal of Public Health found Hispanic patients, those below the poverty threshold, and Medicaid recipients were more likely to delay care due to transportation. Offering remote scheduling and virtual appointment options directly closes that gap.
Service 2: Triage: Every Patient Gets the Right Guidance. Every Time. Not Just When the Right Person Answers.
Triage is one of the highest-stakes services in your operation and one of the most inconsistently delivered. When triage depends on whoever picks up the phone, the quality of the guidance your patients receive varies with the experience and attention level of the individual who answered. That is a clinical risk, not just an operational one.
Your triage operation should be protocol-driven, documented, and consistent across every interaction. Non-clinical staff need tools that guide them through symptom assessment without requiring clinical judgment from every agent: a staff copilot walks your front-desk and administrative team through structured symptom protocols step by step, so every patient gets consistent guidance regardless of who answers. For your clinical staff, a clinical nursing tool surfaces the right patient information at the right moment and documents the result automatically, so your nurses spend their time on clinical judgment rather than chart reconstruction.
This is also where patient safety lives. Your staff will encounter emergencies remotely. A patient presenting with chest tightness during a refill call. A behavioral health contact that escalates. A pediatric call that changes direction mid-conversation. The quality of your safety infrastructure determines what happens in those moments.
Your triage tools should include NLP-driven symptom algorithms that flag clinical red flags in real time, structured urgency classification that routes each contact to the appropriate response level, and one-click escalation that transfers a call directly to an on-call nurse or provider without the patient having to re-explain their situation. For patients whose location is unknown or who cannot provide an address, geolocation integration ensures that if a call requires emergency dispatch, the system gets the correct 911 center on the line without relying on the patient to initiate it.
Every staff member who handles patient interactions, clinical or non-clinical, should be trained in your escalation protocols and practice simulated emergency scenarios. That training is not a formality. It is the infrastructure behind your safety record.
Service 3: Telemedicine: Your Providers Walk Into Every Visit Ready. Your Patients Never Have to Repeat Themselves.
The video visit is the service most practices built first, and for good reason. It is the most visible expression of telehealth, the most directly reimbursable, and the service that most closely mirrors what patients already understand as a clinical encounter.
What most practices underestimate is how much the quality of a telemedicine visit depends on what happens before and after it. A provider who enters a video visit without current patient context, who has to ask a patient to repeat symptoms they already described during intake, who cannot document in real time and have that documentation write back to the EHR automatically: that provider is delivering a technically compliant telemedicine visit inside an operationally broken workflow.
Every telemedicine visit in a complete operation starts with full patient context already in the chart and ends with a documented next step sent to the patient before the session closes. When those two conditions are met consistently, the visit performs at its full clinical and financial potential.
On the regulatory side: the Consolidated Appropriations Act of 2026, signed February 3, 2026, extended Medicare telehealth flexibilities through December 31, 2027. Medicare patients can receive telehealth services from home with no geographic restrictions. Audio-only visits remain covered for eligible services when clinically appropriate. These are statutory extensions and should no longer be referred to as temporary.
Service 4: Medication Refill Management: Requests Stop Piling Up. Patients Stop Waiting. Staff Stop Chasing.
Refill requests are among the highest-volume patient contacts in most practices, and among the most manually handled. A patient calls or sends a message. Someone on your staff logs it, routes it to the appropriate provider, and waits for a response. The provider approves or denies. Someone communicates back to the patient. The pharmacy is notified. In many practices, every one of those steps is a separate manual action performed by a separate person.
When refill management is not automated, it creates two problems. The first is staff load: high-volume, low-complexity tasks that consume disproportionate time. The second is patient experience: delays in refill responses are among the most common drivers of patient dissatisfaction and provider switching.
A complete refill workflow converts every request to a completed outcome: approved, communicated to the patient, and pharmacy-notified, with the provider involved only when clinical review is genuinely required. The result is a service that completes at higher volume with less staff time consumed at every step.
Service 5: Intake: Your Providers Have Full Context Before the Visit Starts.
Intake is the service that most practices consider complete because the forms exist. The forms are not intake. Completed intake means the patient’s information is collected, verified, and available to every staff member and provider involved in their care, before the visit begins, without anyone having to ask the patient to repeat themselves.
Marcus knows his clinical outcomes are strong. His providers are excellent. His patient satisfaction scores inside the visit are high. What his patients experience before the visit, and after it, is a different story entirely. His intake process was a PDF emailed after scheduling confirmation. Half of his patients arrived with it incomplete. The other half completed it on paper in the waiting room. Neither version was in the chart when the provider walked in.
A completed intake workflow means the patient receives a mobile-accessible intake link immediately after scheduling confirms. It collects everything needed. It writes back automatically. Every provider walks into every visit with a verified, complete patient record already in the chart. No provider starts from scratch. No patient repeats themselves. A unified patient data layer is the mechanism that makes that possible: one record that is current, complete, and accessible to every staff member and provider involved in that patient’s care, without manual re-entry at any step.
Research published in the American Journal of Managed Care found the average in-person visit consumes 121 minutes of a patient’s day, with less than 20 of those minutes spent with a provider. Completed intake is one of the most direct ways to make the time your patients spend with you feel worth the investment.
Service 6: Care Coordination: No Patient Falls Through the Cracks Between Departments.
Care coordination is the service that most visibly exposes whether your practice is running as one system or several. A referral that requires a phone call between departments. A follow-up that falls through because the handoff was manual. A specialist who receives a patient without context from the referring provider. Each of these is a care coordination failure, and each one is felt by the patient.
A complete care coordination workflow means information moves automatically between the people and departments involved in a patient’s care. Referrals are generated, transmitted, and tracked inside the same system that handles scheduling and documentation. Follow-ups are assigned and completed, not assumed. Patients do not have to be the messengers among their own care teams.
When scheduling, triage, intake, and documentation all share a single system, every handoff between departments completes cleanly. No data re-entered. No callbacks to confirm what was already documented. No patient left waiting for two departments to talk to each other.
Service 7: Capacity Optimization: Your Schedule Earns at Full Capacity. Even When Things Go Sideways.
An empty appointment slot is not a neutral event. It is revenue that does not complete, a patient who did not get seen, and a provider whose time was not used. Capacity optimization is the service that makes sure your schedule earns at its full potential, not just on the days when everything goes right.
A complete capacity optimization workflow converts every cancelled slot back to a completed appointment before your staff sees the gap. Waitlist management runs automatically, schedule gaps fill through intelligent routing, and your providers complete visits without needing to be physically in the office. A patient schedule change does not have to mean lost revenue. It means an opportunity your system fills before anyone has to ask.
A mature telehealth operation also adapts when the unexpected arrives: a staff shortage, a severe weather event, or any disruption. Your care delivery continues because it is not dependent on everyone being in the same building at the same time.
Service 8: Payment Estimates: Patients Know What They Owe Before They Leave. Collections Follow.
Patients who receive unexpected bills are less likely to pay them and less likely to return. Payment transparency is not a billing department concern. It is a patient experience concern, and it belongs in your telehealth operation alongside every other service that affects how your patients experience care.
A complete payment workflow gives patients an accurate estimate of their out-of-pocket responsibility before or at the time of service. It offers multiple payment channels, including digital payment at point of care. And it integrates with your billing and EHR systems so that what was collected and what was charged are reconciled automatically, without a manual audit process.
When payment is completed at the time of service, your collections improve, your billing cycle shortens, and your patients leave the encounter without an open financial question hanging over the care they just received.
Service 9: Remote Monitoring: Your Clinical Relationship With Patients Continues Between Visits.
Remote patient monitoring is the service that extends your clinical relationship with patients between visits. For practices managing chronic conditions, post-surgical recovery, or high-risk populations, it is also the service with the clearest impact on outcomes.
When patient data, such as vital signs, weight, blood pressure, glucose levels, or physical activity, is transmitted to your care team between encounters, two things happen. Your providers have context they would not otherwise have until the next scheduled visit. And your patients are more engaged in their own care, because the monitoring itself reinforces that someone is paying attention.
Remote patient monitoring requires integration with your EHR so that patient data arrives in the chart continuously, giving your providers current context before every encounter rather than relying on what a patient remembers to report. When that integration is complete, monitoring is not a separate workflow. It is a steady stream of completed clinical inputs that your care team already has when they need them.
Service 10: Patient Engagement: Your Practice Grows From Strategy, Not Just Whoever Calls That Week.
Demand management is the service that most practices have never formally named, which is part of why so few have built it deliberately. It is the capacity to anticipate patient needs, reach patients proactively, and shape the volume and timing of demand on your operation rather than simply responding to it.
In practice, this looks like automated recall outreach for patients who are due for preventive visits. Proactive follow-up for patients who were seen but have not yet completed a recommended next step. Campaign-driven appointment booking tied to specific clinical initiatives. Patient engagement tools that keep your practice present in a patient’s life between visits, rather than invisible until the patient decides to reach out.
A research brief from Altarum calculated that travel and wait time for healthcare cost Americans an estimated $89 billion annually. Much of that cost is driven by fragmented, reactive care: patients who only engage with the healthcare system when something goes wrong, because no proactive outreach reached them first. Demand management is the service that changes that pattern.
When demand management is built into your telehealth operation, your schedule fills with completed appointments driven by clinical strategy, not just whoever called that week. Your providers see the patients who need to be seen. Your preventive visit rates improve. Your recall outreach converts to booked appointments. And your practice grows from a deliberate plan rather than the volume that happens to show up.
What Your Telehealth Stack Needs to Support All Ten Services
Ten services running in isolation are still ten problems. What makes a complete telehealth operation functional is how the services connect.
Practice Management integration. Your scheduling rules, provider requirements, and appointment types need to be automated into every patient interaction. Without PM integration, telehealth workflows become siloed from your core operations.
EHR integration. Your telehealth tools should pull patient context from the EHR before every interaction and write results back to it afterward. Without that bidirectional flow, your staff re-enters data manually, your providers make decisions without current patient history, and your documentation degrades with every interaction not written back to the chart automatically.
Computer-Telephony Integration (CTI). Audio-only telehealth still handles the highest volume of patient contacts in most practices. CTI brings your phone channel into the same unified interface as your other telehealth tools, enabling consistent documentation, lower handle times, and seamless channel transitions mid-interaction.
White-label patient-facing tools. Every patient-facing touchpoint should carry your brand. Self-service that looks like your practice builds trust. Self-service that looks like a third-party vendor builds hesitation.
CRM and campaigns integration. Your demand management and patient engagement workflows should run from the same system that manages scheduling and documentation. That is how campaign-generated contacts convert to completed appointments without manual handoff.
Where the Real Cost Savings Live
The cost side of telehealth gets discussed in terms of technology spend. That is the wrong place to look. Your largest telehealth cost is staff time, and the largest driver of staff cost is the volume of manual work your team performs to complete every patient interaction.
Every step in your patient access workflow that requires a human to initiate it manually is a cost. When those steps are automated, your staff handles the interactions that genuinely require human judgment. Your completion rate per staff hour improves. Your schedule runs at a higher fill rate without proportional headcount increases.
Cross-training with a unified platform also means that when your scheduling queue backs up, trained staff from other functions can step in without a separate login, a separate system, or a separate training cycle. Your overhead scales with volume rather than with department boundaries. The platform’s per-completed-appointment pricing model means your cost scales with the outcomes your operation actually produces, not the volume of attempts it takes to get there.
Key statistics:
- 71.4% of physicians used telehealth weekly in 2024, up from 25.1% in 2018. (AMA, 2025)
- 38x increase in telehealth utilization vs. pre-pandemic baseline, with utilization remaining structurally higher. (McKinsey, 2021)
- 80%+ of patients report they would use telehealth again after a positive experience. (Column Content, 2025)
Your Telehealth Operation Has a Maturity Stage
No practice goes from fragmented workflows to a fully coordinated telehealth operation in one step. The Keona Patient Service Maturity Model maps the progression your operation follows as it develops from inconsistent service delivery to a scaled, AI-coordinated patient access infrastructure.
Marcus, when he finally ran the assessment, landed at Stage 2. Coordinated in some areas, still manual in most of the others. That was not a failure. It was a starting point.
Stage 1: Standardize Care. Scheduling rules, triage protocols, and intake workflows are documented and consistent. Every staff member follows the same process. This is where operational reliability begins.
Stage 2: Coordinate Care. Departments share information in real time. Scheduling, triage, and intake talk to each other. Patient context flows between touchpoints without manual re-entry.
Stage 3: Automate CareFlow. Completion-critical workflows run automatically: appointment confirmations, waitlist fills, intake collection, refill routing. Staff handles escalations. Software handles volume.
Stage 4: Engage Everywhere. Your operation delivers consistent service quality across every channel: phone, web, mobile, patient portal, and text. Patients complete their needs on their terms, without friction.
Stage 5: Scale Excellence. AI anticipates patient needs before they are expressed. Demand management, proactive outreach, and predictive capacity optimization run continuously. Your operation learns and improves with every interaction.
Most practices operating today are somewhere between Stage 1 and Stage 3.
Take the maturity assessment here
What a Complete Operation Actually Feels Like
Marcus went back to his team six months after that Monday morning at the nurses station. Not with a new platform pitch. With a question: of the ten services a complete telehealth operation requires, how many are we actually completing without a human manually intervening at some point?
The answer was three.
That is where the work started. Not by replacing what was there, but by connecting it. Scheduling rules automated into every patient interaction. Triage protocols built into the intake flow. Documentation written back to the chart automatically. Refill requests routed without landing in a shared inbox first.
Eight months later, his front desk was handling a higher volume with the same headcount. His after-hours calls were turning into completed requests without voicemail. His Monday mornings were quieter.
Here is what that looks like in practice: a patient calls at 7:40 PM because her child has had a fever for two days and she is not sure whether it warrants an urgent visit. The call is answered. The symptom protocol runs. The clinical risk is assessed. She is offered a video triage appointment for 8:00 PM. She confirms. Intake is completed via text link before the visit starts. Her child is seen. The provider documents in real time. A follow-up appointment is scheduled before the call ends. The parent does not call back the next morning to ask about next steps, because the next steps were clear, sent to her phone, and scheduled before she hung up.
That interaction did not require more staff. It required a system that knew what to do at every step and completed each one without manual intervention.
That is the operational standard a complete telehealth operation reaches. And it is the standard that CareDesk is built to deliver, across 15 million patient interactions and counting.
See how CareDesk completes 95–99% of patient access across every channel
Frequently Asked Questions: Telehealth Operations
What is the difference between telehealth and telemedicine?
Telemedicine refers specifically to provider-to-patient clinical visits conducted remotely, most commonly over video. Telehealth is the broader category: per the Health Resources and Services Administration, telehealth includes any use of electronic and telecommunications technology to support long-distance clinical health care, patient education, and health administration. Scheduling, triage, remote patient monitoring, medication management, and patient intake are all telehealth services. Your video visit platform is one component of a complete telehealth operation, not the whole thing.
Are Medicare telehealth flexibilities still in effect in 2026?
Yes. The Consolidated Appropriations Act of 2026, signed February 3, 2026, extended all major Medicare telehealth flexibilities through December 31, 2027. This includes home as an eligible originating site with no geographic restrictions, expanded provider eligibility, audio-only telehealth for eligible services, and deferred in-person requirements for behavioral health telehealth. These are statutory extensions, not temporary COVID waivers. For the current policy overview, see telehealth.hhs.gov →
What HIPAA requirements apply to telehealth platforms in 2026?
The HIPAA enforcement waivers that permitted use of non-compliant consumer platforms expired in August 2023. Full HIPAA compliance is required for all telehealth delivery today, including the 2024 Security Rule updates. Every platform in your telehealth stack that handles Protected Health Information must have a signed Business Associate Agreement (BAA). For current guidance, see: HHS HIPAA Security Rule →
How do I know which of the ten services to prioritize first?
Most practices start with the services that directly affect whether a patient completes their first interaction with your practice. Scheduling, intake, and triage are the three that most commonly determine whether a new patient becomes an established one. If a patient cannot schedule easily, cannot complete intake before the visit, or cannot reach the right level of clinical guidance when they call, the other seven services never get the chance to perform. Once those three are running reliably, the Keona Patient Service Maturity Assessment can help you identify where to start next and will surface your highest-impact gaps based on your specific operation.
How does a healthcare CRM support all ten telehealth services?
A scheduling tool manages appointment slots. A healthcare CRM manages the full patient access workflow across all ten services: from first contact through scheduling, intake, triage, care coordination, documentation, and follow-up. Most completion failures in a telehealth operation happen between services, not within them. A healthcare CRM built for patient access is designed to complete every step of that workflow automatically, connecting each service so nothing falls through the gaps.
What is the Patient Service Maturity Model and how do I assess my current stage?
The Keona Patient Service Maturity Model maps five operational stages from Standardize Care through Scale Excellence. It was developed from 15 million patient interactions across specialties including orthopedics, primary care, urology, pediatrics, and women's health. Most practices operating today are at Stage 2 or Stage 3. The maturity assessment takes approximately ten minutes and produces a stage determination with specific recommendations for your next operational investment.
How have patient access expectations changed in recent years?
Patients now benchmark their healthcare access experience against every other digital interaction in their lives: banking, retail, food delivery. Platforms like Amazon One Medical and Walmart Better Care Services have made on-demand virtual care and behavioral health access available around the clock at accessible price points, through apps and platforms patients already use daily. This has raised the bar for what patients consider acceptable access. Practices that make it easy to reach them, schedule, complete intake, and follow up without friction are the ones patients return to. The clinical quality of your care matters. So does how easy it is to get to it.
Where do most practices lose patients in their telehealth workflow?
Most patient losses happen between services, not during them. A patient who completes a video visit but never receives clear next steps. A refill request that sits in a shared inbox for three days. An intake form that was never completed before the visit, so the provider starts from scratch. These are not clinical failures. They are operational gaps in the handoffs between services. The practices that retain patients are the ones that have closed those gaps, so that every step from first contact to completed care runs automatically, without a patient having to follow up to find out what happens next.




