A scheduled appointment is the easy part. The refill, the provider question, the referral that needs three touches before it closes, that is where access quietly breaks. Those steps are also where the strongest operations pull ahead.
The Harder, Costlier Reality of Requests That Aren’t Quickly Resolved
Most patient access conversations are framed around the call:
- How fast you answer
- How many you handle
- How many you finish on first contact
Those numbers matter, but they describe only the requests that resolve in a single conversation. The harder, costlier reality is everything that does not:
- The prescription refill waiting on a provider
- The referral that needs insurance verification before it can be booked
That work does not end when the patient hangs up. It has to be carried, and too often it gets carried in someone’s head.
The Load is Real and Measurable
About 44% of administrative tasks in general practice are mostly or completely automatable with current technology (Willis et al., BMJ Open, 2020). And physicians already spend close to two hours on documentation and desk work for every hour of direct patient care, with another one to two hours after the clinic closes (Sinsky et al., Annals of Internal Medicine, 2016).
A large share of that load is follow-up work that never got a clear owner. That work sits in inboxes, on sticky notes, in the memory of whoever happened to pick up the phone.
A Queue is the Answer to “Who Owns This Now”
A queue is the simplest possible answer to that question. When a request cannot be closed on first contact, it drops into a queue that owns the follow-through. The request carries a goal timer, so there is a deadline, not just an intention. It is visible to both your self-service and your call-center teams, so when the patient calls back, the next person sees exactly where it stands and can help right then, instead of asking them to start the story over.
The rule lives in the system, not in someone’s head. Nothing falls through the cracks because there are no cracks: every open request has an owner and a clock.
That shift, from “we answered the call” to “the request actually got finished,” is the difference between a deflected contact and a completed one. A request that bounces between three people and never resolves still looks fine on a call-volume report. It does not look fine to the patient, and it does not look fine on a queue.
The Quiet Engine Under the Maturity Curve
This is why queues sit at the center of the Patient Service Maturity Model. The model describes how a patient access operation matures across five stages, from standardizing care to running access as a growth engine.
The quiet engine underneath most of that progression is the queue. It switches on the moment work shifts from “schedule it and hang up” to “make sure it actually gets finished.” The queue stays on through every stage after:
- Coordinating work across channels
- Absorbing repetitive volume autonomously
- Engaging patients on their own terms
- Orchestrating growth
What You Actually Get: Service Levels You Can See
Here is the part that rarely makes a feature list and matters most. Once every kind of request lives in a queue with a goal, you can see your service levels across all of them in one place. Not just average speed of answer on the phone, but how long a refill, a referral, or a new booking actually takes, how many are within goal, how many are slipping, and where.
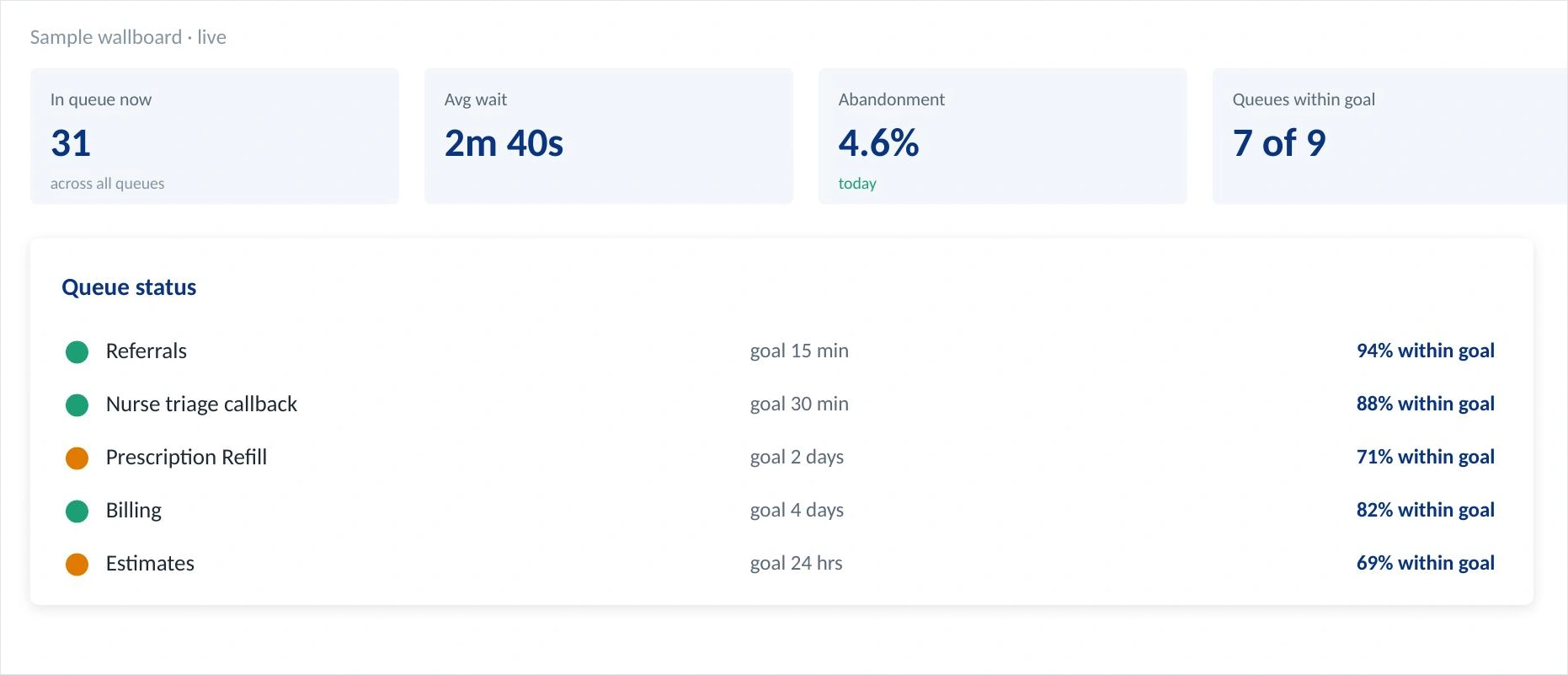
Illustrative service-level view across queues. One place to see in-queue volume, average wait, abandonment, and how many queues are holding their goals.
That single view changes how an operation runs. You stop discovering problems when a patient complains or a referring office goes quiet. You see a queue trending red while there is still time to act. Service levels stop being a phone-system statistic and start being a full picture of whether your operation is keeping its promises.
Referrals: Where Slow Follow-through Quietly Costs You
Consider referrals, where the cost of slow follow-through is easiest to miss. A referral that takes too long to process rarely generates a complaint. It quietly costs you the next referral, because the referring practice notices that their patients wait, and sends the one after that somewhere faster. Put referral processing in a queue with a goal and a per-practice view, and the relationship becomes visible, and protectable.

Illustrative referral queue report. Processing time broken out by referring practice against a two-day goal, so a slipping relationship shows up while you can still act on it. Sample data.
Now the slow relationships are obvious, and so are the strong ones. You can reach the practice drifting past goal before it costs you the relationship your new-patient volume depends on. This is what it means for access to become a growth engine rather than a cost center, and it is the work of the model’s final stage.
The Same Report, Every Team
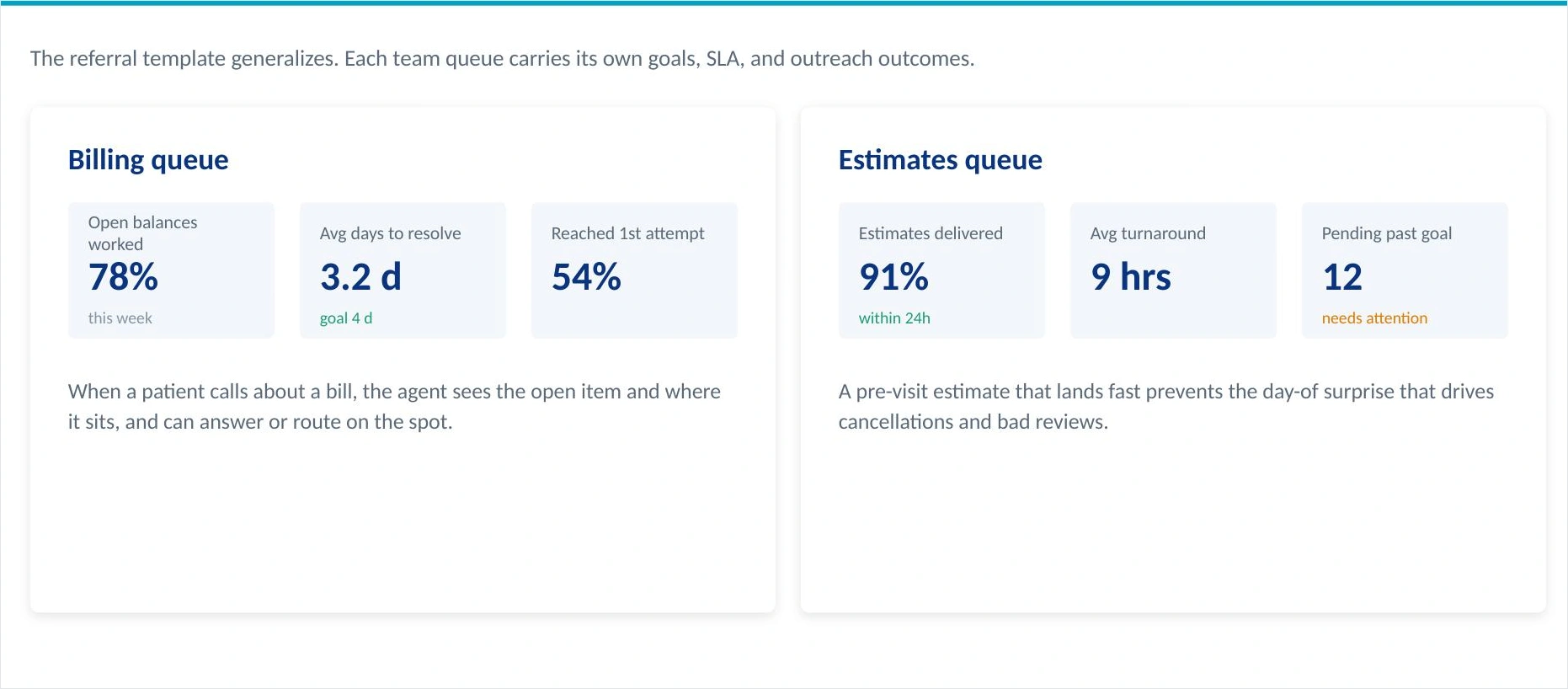
The pattern is not specific to referrals. The same queue report generalizes to every team that owns follow-up work. Billing queues track open balances worked and average days to resolve against a goal. Estimate queues track how fast a pre-visit estimate lands, because an estimate that arrives late is the day-of surprise that drives cancellations and bad reviews.
Each queue carries its own goal, its own service level, and its own outreach history. They all feed one reporting layer.
Illustrative billing and estimates queues. The referral template generalizes: every team queue carries its own goals, service levels, and outreach outcomes.
Where Are You On the Curve?
None of this requires a leap. Each capability is a concrete step, not a transformation program. The question worth asking is simply where your operation sits today: which requests already have an owner and a clock, and which are still being carried in someone’s head. That is the gap worth closing, and it is usually closer than it looks.
See how the five stages map to your operation
The Patient Service Maturity Model lays out the full curve, from standardizing care to running access as a growth engine.You are able to plot where you are and pick the next concrete step.