

This is not a technology failure. It is a sequencing problem. Telehealth was never designed as one integrated system. It was layered on top of workflows that were already fragmented, which means the gaps your team navigates every day are not bugs. They are the predictable result of building capability without building a foundation first.
You invested in telehealth. Your patients can book online, see a provider on screen, and receive follow-up instructions without stepping into your office. And yet, somehow, your phones are still ringing off the hook. Your staff is still toggling between systems. Your schedulers are still cleaning up what the portal left behind.
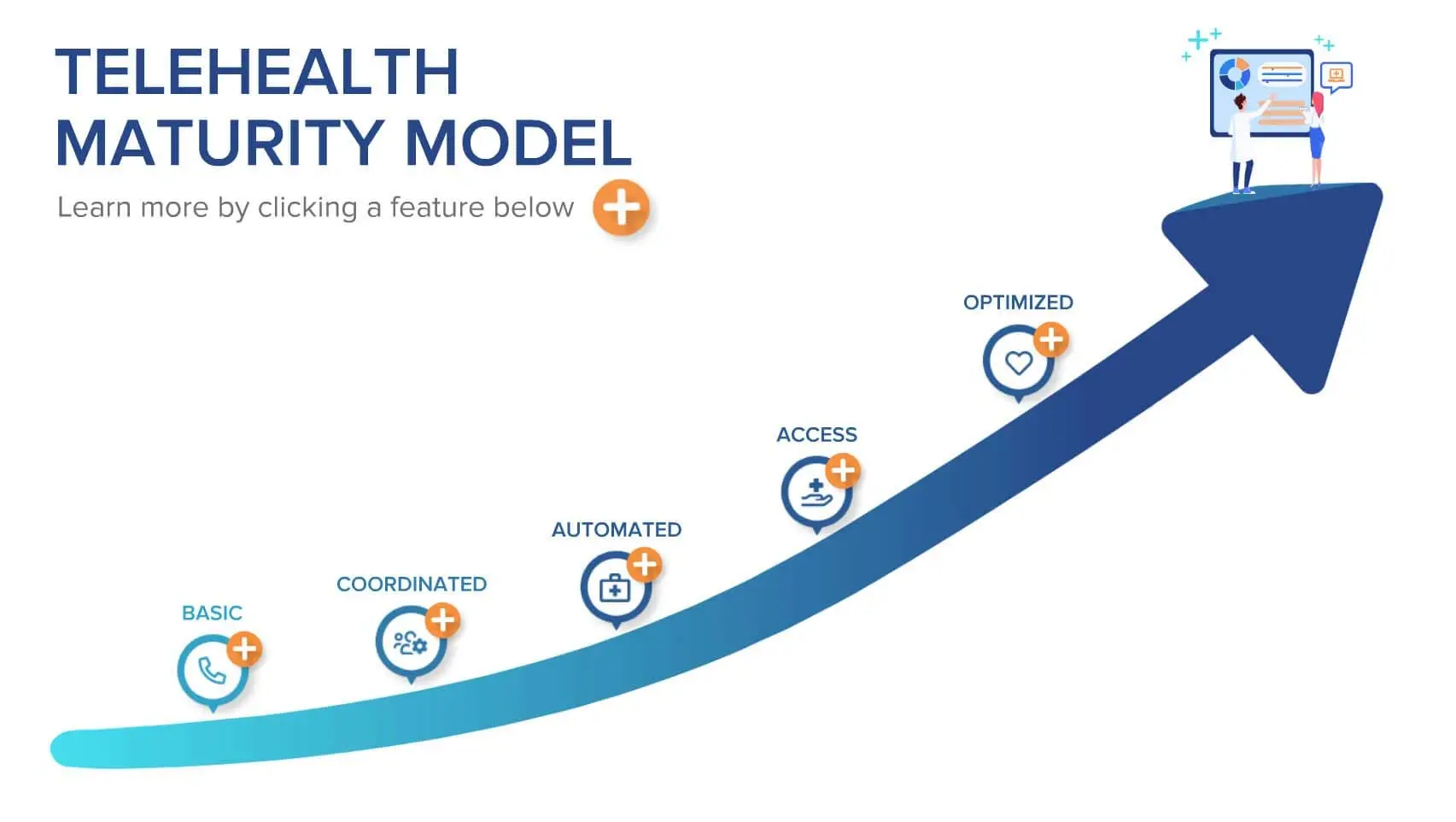
The Telehealth Maturity Model offers a way to think about that progression more clearly. Rather than treating telehealth as a technology problem, it frames the challenge as an organizational one, with five sequential stages that build toward sustainable, high-performing care delivery.
Understanding the Full Reach of Telehealth
When most people in your position hear telehealth, they picture a provider and a patient on a video screen. That is one piece of a much larger picture. As defined by the U.S. Department of Health and Human Services, telehealth encompasses any use of remote technology to support long-distance clinical healthcare. For your operation, that includes:
- Telephone and web-based interactions
- Asynchronous SMS or secure messaging
- Digital scheduling and check-in
- Patient portals and online forms, including photo and image submissions
- Remote patient monitoring
- Administrative preparation and coordination surrounding remote visits
In other words, every digital touchpoint your patients encounter before, during, and after a visit falls within the telehealth umbrella. A smooth virtual visit is not just about the video call. Your patient’s experience depends on your intake, triage, scheduling, documentation, and follow-up processes all working in sequence.
That coordination is what the maturity model is designed to build.
Getting Telehealth Right Means Building It in Stages
A maturity model is a structured roadmap to organizational excellence. It defines the core competencies your team must develop in sequence, helping you break a large transformation into achievable stages rather than trying to change everything at once.
Telehealth transformation follows this pattern. When you try to skip stages, automating before coordinating, or opening patient access before your workflows are ready, you consistently end up with the same result: frustrated patients, overwhelmed staff, and systems that create more work than they eliminate.
The five stages below represent the proven path forward for your operation.
Stage 1: Create a Foundation Worth Building
Align Leadership, Tools, and Standards Across the Practice
Before any coordination or automation is possible, your organization must consolidate. That means aligning leadership, building with a consistent toolset, and establishing a shared set of standards across your departments and specialties.
Without consolidation, each of your departments continues operating on its own terms. Your scheduling lives in one system, triage in another, and intake in a third. Your staff members in different roles are trained differently. Your leadership has no unified view of service quality. Consolidation is what gives your telehealth program a foundation strong enough to build on.
Key practical steps at this stage:
- Establish patient service leadership with cross-department authority
- Consolidate at least three telehealth services onto a single workflow platform
- Implement a Healthcare CRM to manage your patient interactions across time and channels
- Define executive service metrics: net promoter Score, Customer Satisfaction Score, Revenue Growth, Patient Churn
- Build the expertise to document workflows and create consistent training programs across your practice
Centralized vs. federated delivery: what to consider:
As you implement consolidated telehealth, you will need to decide whether to centralize service delivery under one team or federate it across your locations. Centralization is faster to train and easier to implement, but harder to customize for individual providers and locations. Federation takes longer to roll out but allows for more specialty-specific flexibility. Either approach requires that your chosen technology enforces location- and provider-specific requirements at the workflow level, not through staff memory.
Your Healthcare CRM is the anchor for this stage. It brings your patient data together across systems (PM, EHR, telephony, messaging) and creates a unified workspace that makes coordination possible in the next stage.
Stage 2: Connect Every Step in the Patient Journey
Guided by Four Principles of Coordination
Coordination is the most demanding stage in patient care, and also the most consequential. This is where your team maps, documents, and tightly links every step in the patient service journey, so that no step is isolated from what came before or after it.
Keona professor Clayton Christensen noted in The Innovator’s Prescription that healthcare has historically operated in batch processing: each department handles its piece of the work, then passes it to the next, where queues can build. Your patients move between departments, sometimes repeating information and bridging gaps themselves. A mature telehealth operation redesigns this model so that continuity travels with the patient, not the other way around.
The four Principles of Telehealth Coordination:
- Every decision point has full patient context. Documentation travels with your patient. Your staff handling any step can see what happened before and what comes next.
- Each step is aware of the steps before and after. No handoff is blind. Your workflows anticipate what information will be needed at the next step, and they make it accessible to your staff, before, during, and after the telehealth visit.
- All possible services are provided in a single interaction. Transfers and callbacks become exceptions, not defaults.
- Services are connected across every channel. A patient who starts online and finishes by phone does not start over or have to repeat themselves.
To illustrate the impact, here is a disjointed telehealth workflow example: the patient who tries to schedule a visit via an online patient portal, but they have symptoms that need triage. Then once they are booked for a telehealth visit with a provider, it turns out they needed a specialist referral, and they start over and wait while that step is figured out.
That sequence could have involved more than a dozen separate interactions across your staff, and it still wasn’t smooth for the patient. The coordinated version of the same scenario, following these four principles, takes four steps. Not because shortcuts were taken, but because the information travels with your patient instead of getting lost at each handoff.
Additional coordination priorities at this stage:
- All staff who interact with your remote patients are trained in telehealth safety, clinical documentation, and soft skills for digital communication
- QA metrics are established for all telehealth roles across your practice, including outcome, flow, and safety KPIs
- Your healthcare tools are integrated into a single staff workspace
- Workflows are documented in a format accessible to all staff across your teams
One example of this principle in action: practices that complete patient intake at the time of scheduling, rather than at check-in, see smoother visits, less waiting room congestion, and fewer provider delays throughout the day. When your scheduling tools, for both telehealth and in-person visits, are designed to support any clinical role, your nurses, medical assistants, and technicians can complete the scheduling interaction without transferring the patient to a dedicated scheduler.
Stage 3: Make Every Interaction Consistent and Safe
Automation Is What Makes It Scale
Automation at this stage does not mean replacing your staff’s judgment. It means taking the coordinated workflows your team built in Stage 2 and embedding them into your tools so that your staff are guided at each step, documentation happens in real time, and safety checks run automatically.
Building this foundation is what makes patient-facing self-service successful for your practice. When your workflows are embedded in the tools, your patients experience the same guided, consistent journey that your staff relies on, with the same safety checks running in the background.
Priority automation areas for your operation:
- Workflow triggers built around your visit types, specialties, providers, and insurance requirements
- Automated encounter routing based on your staff’s skill sets and training levels
- A context-sensitive Knowledge Base that delivers relevant information to your staff based on the patient, call type, specialty, and location, without requiring a manual search
- Safety and escalation logic, including clinical decision support, natural language symptom algorithms, on-call routing, E911 integration, and geolocation-based emergency mapping
- Real-time capture of encounter metrics across every channel your practice uses: total handle time, steps per resolution, average speed to answer, complaint volume
Embedding safety into your digital workflows is one of the most meaningful things Stage 3 accomplishes. When escalation logic, clinical decision support, and emergency routing are built directly into your tools, every patient interaction carries the same protective scaffolding that your in-person and phone encounters have always had. That consistency is both a clinical and a competitive asset for your practice.
Stage 4: Give Patients the Access They Expect
Self-Service That Is Safe Enough to Trust
When your first three stages are complete, your practice has the workflow infrastructure it needs to extend that same guided, consistent experience directly to your patients. Stage 4 is where that happens.
Your patients’ demand for digital access is not a trend. It is a durable expectation. According to Experian Health, 89% of patients say the ability to schedule appointments anytime using digital tools is important. Yet only 63% of providers had plans to implement self-scheduling options. That gap is both a patient experience risk and a competitive one for your practice.
The J.D. Power 2024 U.S. Telehealth Satisfaction Study found that 65% of telehealth patients encounter at least one barrier during their visit, most commonly connectivity issues, limited services, or data security concerns. A mature digital access stage removes those barriers from your patients’ experience systematically, not by chance.
What this stage looks like in your practice:
- Your patients have self-service access to scheduling, symptom assessment, health education, intake, check-in, and billing. Each function has safety checks and escalation logic built in
- Your patients can move between channels (web, phone, text, secure messaging) without losing their prior work or repeating information
- Your pricing and/or insurance coverage and billing process is transparent
- Patient-reported and cross-channel KPIs are captured for your operation, including satisfaction ratings, channel preference by demographic and specialty, wait time per channel, and escalation rates
Remote vs. localized telehealth staff workflows:
At this stage, you also need to plan for the full range of telehealth staffing configurations that your practice may use. In localized telehealth, your patients are remote, but your staff works in a shared physical location, making coordination easier. In remote telehealth, both your patients and your staff are distributed.
Remote telehealth requires more rigorous process documentation, more mature collaboration tools, and deeper automation of handoffs. When your staff can work remotely, your practice gains flexibility during unexpected disruptions, such as extreme weather, local outbreaks, and surges in demand. Building this capability now creates resilience for situations that will eventually arrive.
Stage 5: Use Data to Drive Continuous Improvement
From Reactive to Proactive Care Delivery
Stage 5 is where your telehealth program becomes a genuine competitive
differentiator. Your practice at this stage has the data, workflows, and staff
depth to forecast demand, detect population-level trends, and continuously
improve every channel in real time.
This is also the stage that unlocks what may
be the most underutilized capability in specialty healthcare: demand management.
Rather than reacting to your call volume and appointment gaps, your practice
shapes demand, directing patients to the most appropriate channel, visit type,
or care pathway based on real-time conditions.
Stage 5 capabilities for your operation:
- Syndromic surveillance: reporting tools map symptom data by ZIP code and patient population, allowing your team early detection of health trends and timely reporting to public health boards
- Demand forecasting: models built from your cross-platform data account for seasonality, channel use patterns, and clinical trend cycles, including flu season timing and post-holiday care surges
- Continuous channel optimization: the relative use, effectiveness, and outcomes for each of your channels are measured against your local population needs and adjusted accordingly
- Holistic patient experience KPIs: net promoter score, first contact resolution, customer satisfaction score, mean time to resolve, and complaint volume, reviewed on a continuous basis across your practice
- Satisfaction guarantees: with deep knowledge of service capabilities and adaptability, some practices at this stage offer formal service commitments, an approach associated with stronger patient retention and competitive differentiation
The adaptability that comes with Stage 5 is not theoretical. Your practice at this stage can respond to an unexpected outbreak by standing up a new digital assessment workflow in hours, not weeks. You can create new visit types, customize them by provider, and push them live without rebuilding from scratch. This is the payoff for doing the earlier stages correctly.
What Mature Telehealth Delivers for Your Practice and Your Patients
When your practice reaches telehealth maturity, the outcomes extend well beyond the virtual visit itself. According to the Doximity 2024 State of Telemedicine Report, 64% of physician telemedicine users reported improved patient outcomes, and nearly 84% said telemedicine has increased patient satisfaction. Among patients who used virtual care in the past year, 96% rated their overall care the same or better than in-person visits.
For your patients, maturity means:
- Faster access to care, with fewer transfers and callbacks
- Greater choice of channel without losing continuity
- Reduced total cost of the visit
- Easier navigation, especially for your elderly patients and parents of pediatric patients
- Better chronic disease management through more consistent follow-up
For your practice, maturity means:
- Increased revenue from reduced leakage and higher scheduling efficiency
- Greater schedule flexibility across in-person, virtual, and hybrid visit types
- Improved continuity of care across your full patient journey
- Organizational resilience when unexpected disruptions arise
- The competitive positioning to retain and attract patients who expect a modern access experience
Taking the First Step Toward Mature Telehealth
Your practice likely already has a sense of where it stands, even without a formal framework to describe it. You may have already discussed that there is room to tighten handoffs between your teams, bring your scheduling tools into a single workspace, or give your patients more digital options for reaching you. The maturity model gives those instincts a name and a sequence.
Each stage builds directly on the one before it. The practices that have committed to this progression are not just delivering better virtual care. They are more adaptable, more resilient, and better positioned for whatever comes next in a healthcare landscape that is still changing rapidly.
Telehealth is no longer an alternative channel for your practice. According to SecureVideo, it is now a permanent pillar of healthcare delivery. The question is no longer whether to offer telehealth. The question is how mature your operation is to support it.
Ready to map your telehealth maturity? See where you stand.
Frequently Asked Questions About Telehealth Maturity
What is a telehealth maturity model?
A telehealth maturity model is a structured framework that defines the stages your organization must move through to deliver excellent virtual care. Rather than treating telehealth as a single technology deployment, the model recognizes that sustainable performance depends on building the right organizational capabilities in the right order: consolidating your leadership and tools, coordinating your workflows, automating for consistency, enabling patient self-service, and ultimately optimizing through data. Skipping stages typically leads to fragmented experiences, staff burnout, and patient dissatisfaction.
How large is the telehealth market in 2026?
The global telehealth market is growing rapidly. Fortune Business Insights projects the global market to reach approximately $1.27 trillion by 2034, expanding at a compound annual growth rate of around 24.6%. North America holds the largest regional share, and the U.S. market alone was valued at roughly $42 billion in 2024. Adoption of AI-powered telehealth tools to support this is also growing, per Fortune Business Insights, driven by intelligent triage, contact center automation, and remote patient monitoring.
Why do so many telehealth implementations underperform?
Most telehealth underperformance is solvable, and it typically traces back to one of two causes. The first is telehealth programs built without a foundation of patient care coordination. The second is opening the door to patient-facing access before your workflows are automated. When your staff workflows are still siloed, self-service options can surface the same friction points your patients were already encountering by phone. The J.D. Power 2024 U.S. Telehealth Satisfaction Study found that 65% of telehealth patients experienced at least one barrier during their visit. Enhancing the maturity of your practice’s telehealth workflow, not technology alone, is what removes those barriers from your patients’ experience.
What are the four Principles of Telehealth Coordination?
The four principles are: (1) every decision point has full patient context, (2) each step in your workflow is aware of the steps before and after it, (3) all possible services are provided in a single interaction to minimize transfers and callbacks, and (4) your services are connected across every channel so your patients do not repeat themselves when switching between phone, web, text, or video. Practices that apply these principles consistently see dramatic reductions in the number of steps required to deliver care to a patient in a telehealth visit.
What is demand management in a mature telehealth practice?
What role does AI play in telehealth maturity?
AI becomes most valuable to your practice and telehealth offering once the foundational stages of patient care coordination and automation are in place. In a mature telehealth program, AI powers clinical decision support, natural language symptom algorithms, and escalation logic across your workflows. In more advanced practices, AI enables your patients to safely navigate symptom assessment, scheduling, and care coordination on their own. At the highest performing practices, AI drives population-level trend detection and demand forecasting for your operation. According to Dash Tech, AI in 2026 has moved well beyond pilots into embedded clinical and operational workflows, and the meaningful distinction now is between organizations with governed, interoperable AI and those still working toward it.
How does patient self-scheduling fit into telehealth maturity?
Self-scheduling is an important capability for your practice, but one that is not a quick fix, and introducing it too early can lead to disappointment. According to Experian Health, 89% of patients say anytime digital scheduling is important to them. But deploying self-scheduling before your workflows are coordinated and automated tends to create patient-facing friction that mirrors the internal friction your staff were already experiencing. The technology works best when your underlying system works first. That is why successful practices build a telehealth program through the several maturity stages in order.




